Bone Age in Girls Aged 7 Years — Greulich-Pyle Hand and Wrist X-Ray Reference
Bone age assessment using a left hand and wrist radiograph is a fundamental tool in pediatric radiology for evaluating skeletal maturity relative to chronological age. The Greulich-Pyle (GP) method compares a child’s radiograph against standardized atlas plates derived from a North American reference population. In 7-year-old girls, accurate bone age estimation guides workup for growth disorders, precocious puberty, endocrine abnormalities, and, when needed, medicolegal age estimation.
Expected Ossification Centers and Skeletal Findings
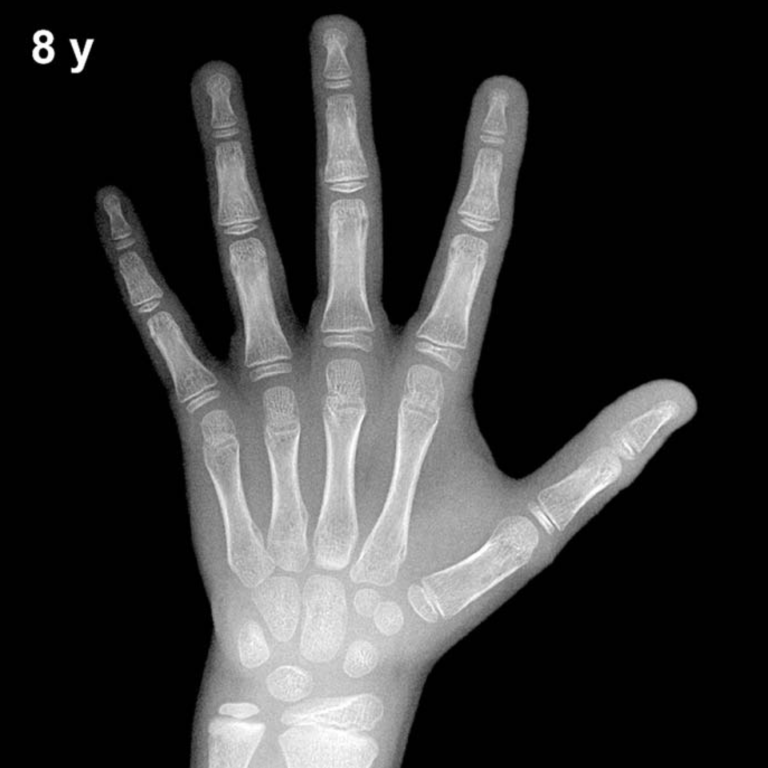
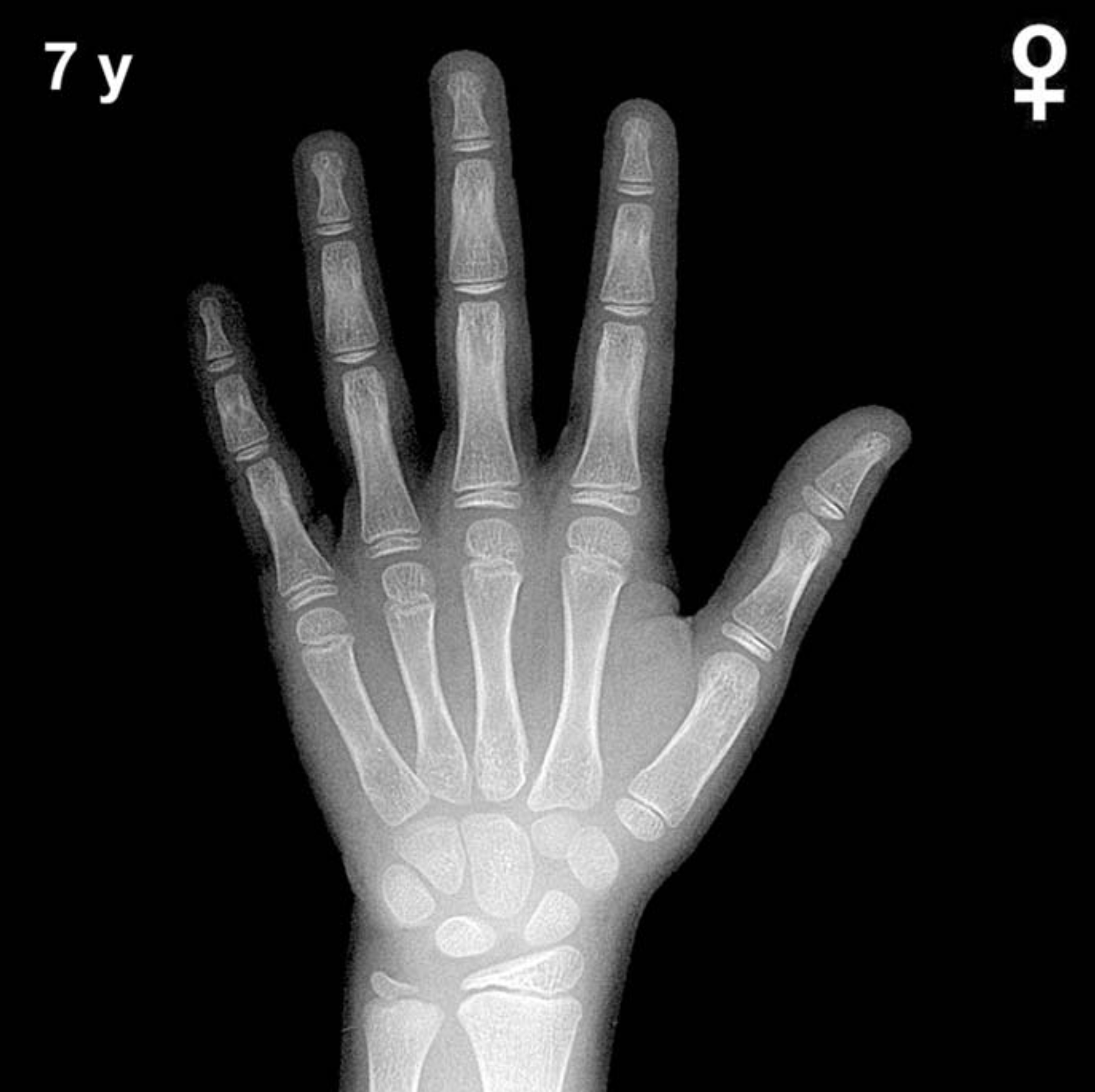
By 7 years of age in girls, all primary carpal ossification centers are typically visible. The capitate and hamate (appearing around 3 and 6 months, respectively) are well established and increasing in size. The triquetrum, appearing around 2–3 years, and the lunate, around 3–4 years, should be clearly ossified. The scaphoid, trapezium, and trapezoid — typically appearing between 4 and 6 years — are expected to be present and well-defined by this age in girls.
The distal radial epiphysis (appearing around 1 year) is well developed by age 7, showing progressive widening and increased density. The distal ulnar epiphysis, which typically appears between 5 and 7 years, may be present or just emerging at this age in girls. Epiphyses of the metacarpals and phalanges are present and show progressive capping. The pisiform, which typically appears between 9 and 12 years in girls, is generally not yet expected at age 7. Similarly, the adductor sesamoid of the thumb is a peripubertal landmark not expected at this age.
- Capitate and hamate: well ossified
- Triquetrum, lunate: present and defined
- Scaphoid, trapezium, trapezoid: typically visible by age 7 in girls
- Distal radial epiphysis: well developed
- Distal ulnar epiphysis: emerging or present
- Pisiform and thumb sesamoid: not yet expected
Clinical Pearls
Girls consistently demonstrate skeletal advancement compared to boys of the same chronological age, often by approximately 1–2 years across mid-childhood. At age 7, a bone age within ±1 year (i.e., 6–8 years) is generally considered within the normal range of variation, reflecting one standard deviation in the GP reference population. A bone age significantly advanced beyond this range may prompt evaluation for precocious puberty, obesity-related early maturation, or congenital adrenal hyperplasia. Conversely, a notably delayed bone age warrants consideration of growth hormone deficiency, hypothyroidism, or constitutional delay of growth and puberty.
A key interpretive pitfall is relying solely on a single carpal or epiphyseal landmark rather than assessing the overall pattern of the hand and wrist. Population differences from the original GP reference cohort may also lead to systematic over- or underestimation in certain ethnic groups; clinical context should always complement the radiographic assessment. Reference: Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development of the Hand and Wrist. 2nd ed. Stanford University Press, 1959.