Bone Age in Girls Aged 17 Years — Greulich-Pyle Hand and Wrist X-Ray Reference
Bone age assessment using a left-hand and wrist radiograph provides a reliable estimate of skeletal maturity, most commonly interpreted against the Greulich-Pyle atlas standards. In adolescent girls aged 17 years, this evaluation is particularly relevant in the workup of growth disorders, delayed or arrested puberty, and forensic age estimation. Accurate bone age interpretation at this late adolescent stage helps clinicians determine whether skeletal maturation is on track for physiological epiphyseal fusion.

Expected Ossification Centers and Skeletal Findings
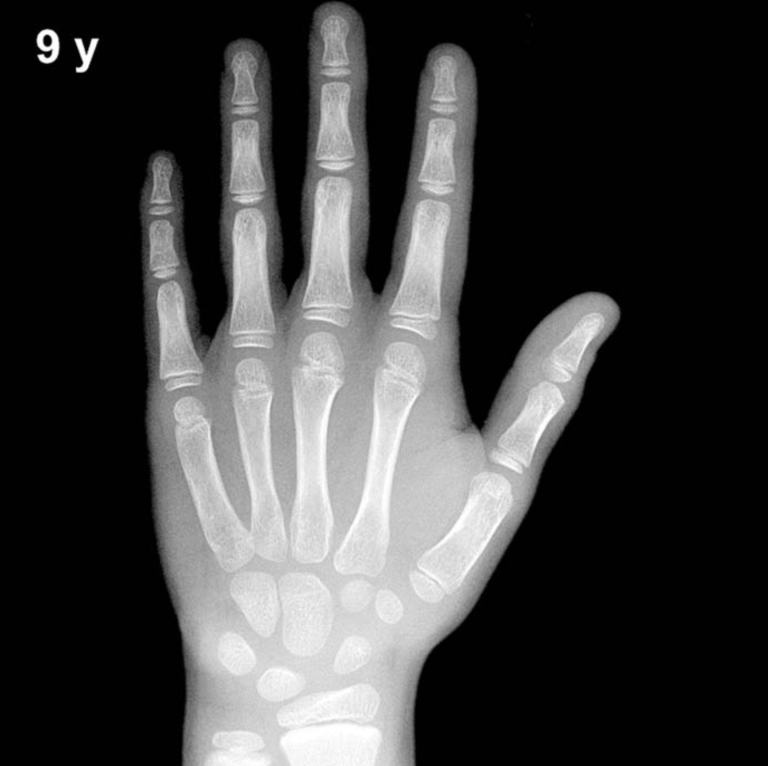
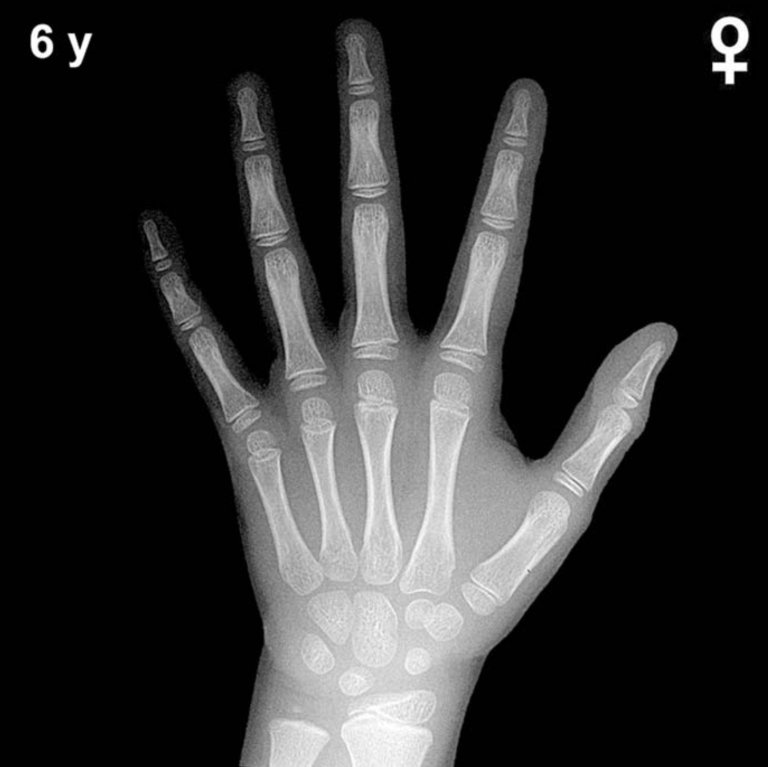
By 17 years in girls, all primary carpal ossification centers are well established and mature. The capitate, hamate, triquetral, lunate, scaphoid, trapezium, trapezoid, and pisiform are fully ossified and adult in morphology. The pisiform, which typically appears between 9 and 12 years in girls, is expected to be fully formed and well-corticated by this age.
The key skeletal hallmark at 17 years in girls is progressive or near-complete epiphyseal fusion across the hand and wrist. Fusion of the distal radial and ulnar epiphyses is typically underway or complete, and epiphyses of the metacarpals and phalanges are expected to be fused or in advanced stages of fusion. The adductor sesamoid of the thumb, which appears peripubertally (typically around Tanner stage 3 in girls), is fully ossified and well-defined by this age.
- Carpal bones: All eight carpals ossified and mature in contour.
- Distal radius and ulna: Epiphyseal fusion complete or near-complete.
- Metacarpal and phalangeal epiphyses: Fused or showing advanced fusion, particularly in the proximal and middle phalanges.
- Thumb sesamoid: Fully ossified; its absence at this age would be atypical.
Clinical Pearls
At 17 years, a bone age concordant with chronological age reflects timely skeletal maturation consistent with normal pubertal progression in girls. A bone age significantly advanced beyond 17 years (approaching 18–19 years with complete fusion) may indicate prior exposure to excess sex steroids, such as in treated or untreated precocious puberty. Conversely, a notably delayed bone age — with open epiphyses and immature carpal morphology — raises concern for hypogonadism, growth hormone deficiency, hypothyroidism, or chronic systemic illness. Turner syndrome (45,X) should remain in the differential for girls presenting with short stature and delayed skeletal maturation at any age. A key interpretive pitfall at this stage is over-reliance on single-center fusion as a definitive endpoint; fusion sequence varies across bones, and partial fusion lines may persist, particularly at the distal radius, into the late teens. Skeletal age should always be interpreted in the clinical context of growth history, pubertal staging, and relevant laboratory findings. Reference: Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development of the Hand and Wrist. 2nd ed. Stanford University Press, 1959.