Bone Age in Boys Aged 18 Months — Greulich-Pyle Hand and Wrist X-Ray Reference
Bone age assessment using a left-hand and wrist radiograph is a well-established method for evaluating skeletal maturity in children. The Greulich-Pyle atlas provides age- and sex-matched standards against which an individual child’s radiograph is compared. In boys at 18 months, this assessment is particularly useful when investigating early or delayed growth, endocrine disorders, or when estimating developmental age in clinical or forensic contexts.

Expected Ossification Centers and Skeletal Findings
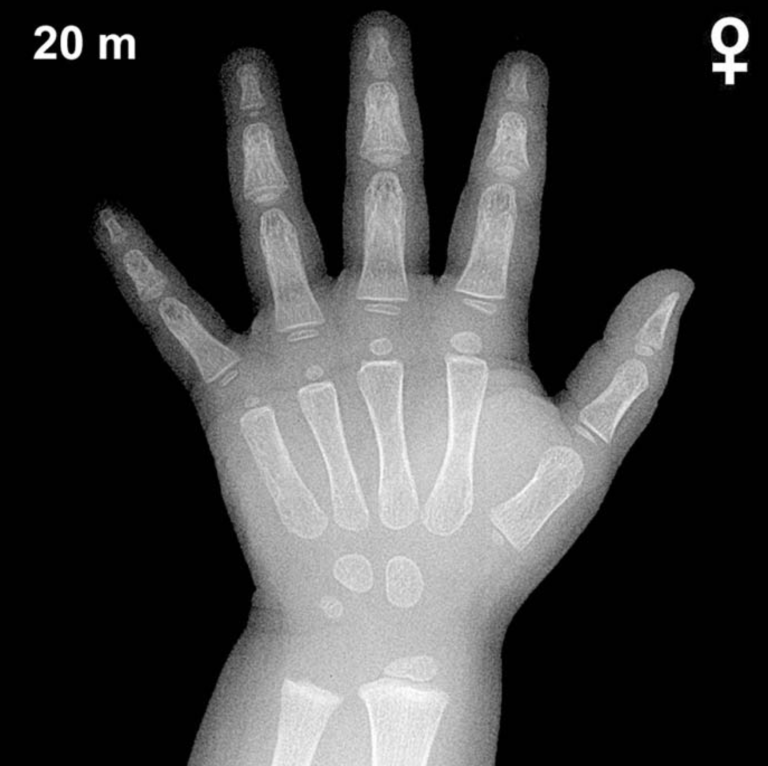
At 18 months in boys, skeletal maturation is still in an early stage, and only a limited number of ossification centers are typically visible on the hand and wrist radiograph. The capitate and hamate are the earliest carpal bones to ossify, appearing around 3 and 6 months of age respectively, and should be well established by 18 months. The distal radial epiphysis typically becomes visible around 12 months and should be present at this age, though it remains small and rounded.
By 18 months in boys, the following findings are generally expected:
- Capitate: ossified and visible (present since ~3 months)
- Hamate: ossified and visible (present since ~6 months)
- Distal radial epiphysis: present, small and disc-like
- Triquetral: typically not yet ossified in boys at this age (usually appears ~2–3 years)
- Lunate, scaphoid, trapezium, trapezoid, pisiform: not expected at 18 months
- Distal ulnar epiphysis: not yet expected (typically appears ~5–7 years)
- Metacarpal and phalangeal epiphyses: beginning to appear, though variable
The overall bone age in boys at 18 months is characterized by relatively few visible ossification centers, reflecting the normal lag in male skeletal maturation compared with girls of the same chronological age.
Clinical Pearls
At 18 months, girls are skeletally ahead of boys by approximately 2–6 months on average, a difference that widens during mid-childhood and peaks around puberty. A bone age significantly advanced beyond 18 months in a boy may prompt evaluation for conditions such as precocious puberty, congenital adrenal hyperplasia, or exogenous androgen exposure. Conversely, a bone age notably delayed relative to chronological age raises consideration of growth hormone deficiency, hypothyroidism, or constitutional delay of growth and puberty. At this young age, the standard deviation for bone age estimates is wide (approximately ±6 months), so mild discrepancies should be interpreted cautiously and always in the context of auxological data and clinical history. A key pitfall is over-relying on a single radiograph in isolation; serial assessments and correlation with growth velocity provide greater diagnostic value. Reference: Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development of the Hand and Wrist. 2nd ed. Stanford University Press, 1959.