Bone Age in Boys Aged 16 Months — Greulich-Pyle Hand and Wrist X-Ray Reference
Bone age assessment using a left hand and wrist radiograph is a well-established method for evaluating skeletal maturity in children. The Greulich-Pyle (GP) atlas provides standard reference plates matched by sex and age, allowing comparison of a child’s radiograph against population norms. In clinical practice, bone age is integral to the workup of growth disorders, precocious or delayed puberty, endocrine abnormalities, and, in some contexts, forensic age estimation.

Expected Ossification Centers and Skeletal Findings
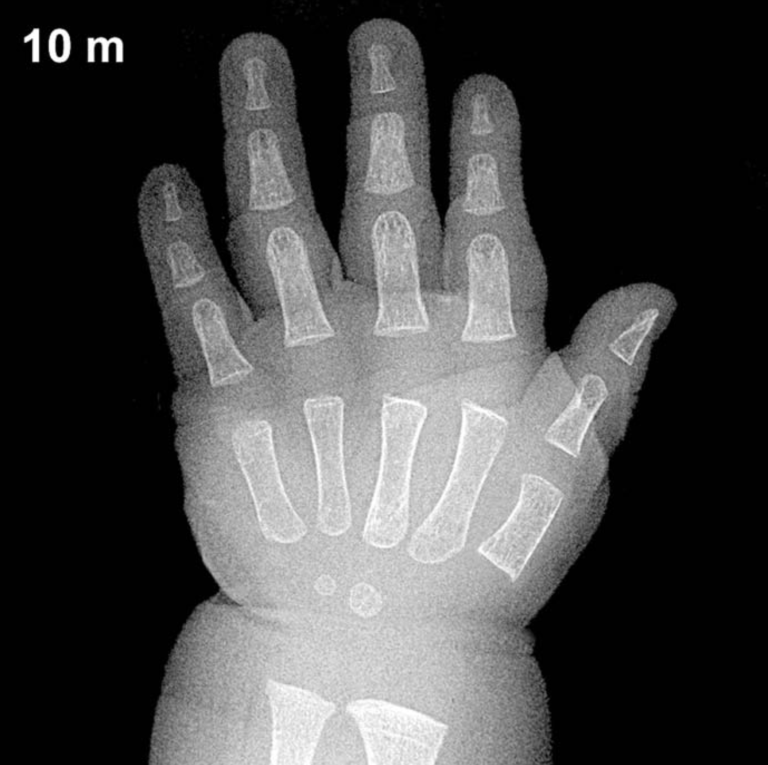
At 16 months of age in boys, skeletal maturation is still in its early stages. The capitate and hamate are typically the first carpal bones to ossify, appearing around 3 and 6 months of age respectively, and should be well established by 16 months. The distal radial epiphysis typically ossifies around 12 months in boys and is generally visible by this age, though its size and definition may still be modest.
The triquetral ossification center emerges between approximately 2 and 3 years in boys, so it is not expected to be visible at 16 months. Similarly, the lunate, scaphoid, trapezium, trapezoid, pisiform, and distal ulnar epiphysis all appear considerably later and would not be anticipated on a 16-month radiograph. The metacarpal and phalangeal epiphyses may be beginning to ossify, with proximal phalangeal epiphyses typically appearing in the first 1–2 years of life.
- Present by 16 months (boys): Capitate, hamate, distal radial epiphysis (typically), proximal phalangeal epiphyses (emerging)
- Not yet expected: Triquetral, lunate, scaphoid, trapezium, trapezoid, pisiform, distal ulnar epiphysis, sesamoid of thumb
Clinical Pearls
Normal skeletal maturation carries a standard deviation of approximately ±2–3 months at this age, so minor variation from the expected GP plate is not inherently pathological. Girls are typically 2–4 months skeletally advanced compared to boys at this age. A bone age significantly advanced beyond 16 months in a boy may prompt evaluation for precocious puberty or exogenous androgen exposure, whereas a notably delayed bone age raises concern for growth hormone deficiency, hypothyroidism, or constitutional delay of growth and puberty. A key interpretive pitfall is over-reliance on a single ossification center: assessment should integrate the overall pattern of carpal and epiphyseal development rather than any one finding in isolation. Reference: Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development of the Hand and Wrist. 2nd ed. Stanford University Press, 1959.